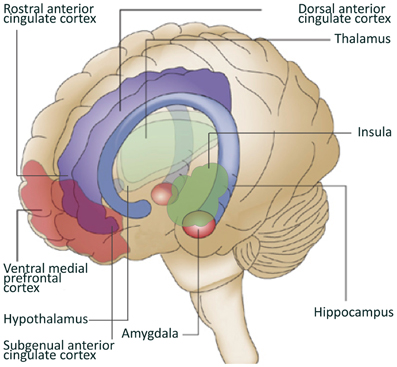
This image is from a different article, "Neuroimaging resilience to stress: A review," Front. Behav. Neurosci., 07 May 2013 | doi: 10.3389/fnbeh.2013.00039.
Resilience has become a buzzword in the health and psychology press, a word generally defined as an individual's ability to adapt to stress or adversity in healthy ways. But it is a much more complex issue than that.
The article below employs a relational developmental systems model to understanding how resilience is formed. Most previous research has focused on the behavioral and psychosocial aspects of resilience. Dante Cicchetti, in the article below, adopts a much more comprehensive model.
The pathway to either psychopathology or resilience is influenced by a complex matrix of the individual’s level of biological and psychological organization, current experiences, active choices, the social context, timing of the adverse event(s) and experiences, and the developmental history of the individual.In seeking to understand how resilience occurs, or doesn't occur, Cicchetti looked at maltreated children using a multilevel analysis to make sense of why some children develop resilience and others develop psychopathology.
Full Citation:
Cicchetti, D. (2010, Oct). Resilience under conditions of extreme stress: A multilevel perspective. World Psychiatry; 9(3): 145–154.
Resilience under conditions of extreme stress: A multilevel perspective
AbstractResilience has been conceptualized as a dynamic developmental process encompassing the attainment of positive adaptation within the context of significant threat, severe adversity, or trauma. Until the past decade, the empirical study of resilience predominantly focused on behavioral and psychosocial correlates of, and contributors to, the phenomenon and did not examine neurobiological or genetic correlates of and contributors to resilience. Technological advances in molecular genetics and neuroimaging, and in measuring other biological aspects of behavior, have made it more feasible to begin to conduct research on pathways to resilient functioning from a multilevel perspective. Child maltreatment constitutes a profound immersion in severe stress that challenges and frequently impairs development across diverse domains of biological and psychological functioning. Research on the determinants of resilience in maltreated children is presented as an illustration of empirical work that is moving from single-level to multilevel investigations of competent functioning in the face of adversity and trauma. These include studies of personality, neural, neuroendocrine, and molecular genetic contributors to resilient adaptation. Analogous to neural plasticity that takes place in response to brain injury, it is conjectured that it may be possible to conceptualize resilience as the ability of individuals to recover functioning after exposure to extreme stress. Multilevel randomized control prevention and intervention trials have substantial potential for facilitating the promotion of resilient functioning in diverse high-risk populations that have experienced significant adversity. Determining the multiple levels at which change is engendered through randomized control trials will provide insight into the mechanisms of change, the extent to which neural plasticity may be promoted, and the interrelations between biological and psychological processes in the development of maladaptation, psychopathology, and resilience.* * * *From the perspective of developmental psychopathology, maladaptation and mental disorder are viewed as evolving from progressive liabilities in the organization of biological and psychological systems, resulting in the undermining of the individual’s efforts to adapt effectively to stressful and adverse experiences 1,2. The dynamic interplay between risk and protective forces is conceived as influencing the developmental course through the impact it has on the quality of the organization of biological and psychological systems as the individual develops 3.Developmental psychopathologists stress that there is multifinality in developmental processes such that the manner in which persons respond to and interact with vulnerability and protective factors at each level of the ecology (i.e., culture, community, family, and their transactions) allows for diversity in developmental outcomes 4,5. Individuals may begin on the same major developmental trajectory, yet exhibit very different patterns of maladaptation or adaptation. The pathway to either psychopathology or resilience is influenced by a complex matrix of the individual’s level of biological and psychological organization, current experiences, active choices, the social context, timing of the adverse event(s) and experiences, and the developmental history of the individual 5.
Understanding the dynamic transactions between risk and protective factors plays a central role in building developmentally informed models of prevention. Through increasing the relative balance of protective processes over risk factors, the potential for righting the developmental course, attaining adaptive developmental pathways, and reducing the emergence of psychopathology may be achieved 4,6.Just as deviations from the average expectable environment potentiate some individuals toward the development of maladaptation, others demonstrate adaptation in the face of the same challenges 7,8,9. Thus, it is equally important to comprehend the mechanisms that promote adaptation among individuals experiencing significant adversity as it is to investigate the developmental trajectories toward maladaptation. Research conducted on biological, as well as psychological, protective factors is critically important for discovering mechanisms and processes that contribute to the development of either the recovery of function or resilient adaptation in the face of significant adversity 10,11,12.DEFINITION AND HISTORICAL CONTEXTResilience is conceived as a dynamic developmental process encompassing the attainment of positive adaptation within the context of significant adversity 8,13,14. There are two critical conditions that are implicit within this conceptualization of resilience: a) exposure to significant threat, severe adversity, or trauma; and b) the achievement of positive adaptation despite major assaults on the developmental process 8,14.For four decades, researchers interested in children who develop well in the context of significant adversity have endeavored to enhance understanding of the diverse pathways to psychopathology, to elucidate the processes that eventuate in normal development, and to inform preventive interventions and social policies that could improve the lives of vulnerable children and families 7,15,16,17,18. Investigations in the area of risk and resilience have led scientists to rethink their prior assumptions about the causes and course of psychopathology and have resulted in a reformulation of the deficit etiological models that characterized earlier viewpoints about the development of children who have experienced disadvantage and great adversity 9,19,20.Studies conducted on individuals at high risk for psychopathology and on persons with mental disorders frequently portrayed the developmental course as deterministic, inevitably resulting in maladaptive and pathological outcomes. Investigations focusing on genetic and biological predispositions to psychopathology, assaults on development associated with inadequate caregiving, and traumatic occurrences within the home – such as child maltreatment and domestic violence, exposure to community violence, chronic illness, and catastrophic life events – graphically convey the multiplicity of risks that can eventuate in disordered outcomes. As researchers discovered that not all high-risk children manifested the dire consequences that extant theories of psychopathology predicted, comprehending the processes through which children at risk did not develop psychopathology became viewed as important for informing theories on the development of maladaptation and pathology.Before investigations on resilience could be initiated, a significant and illustrious history of research detailing the precursors to, as well as the contemporary patterns of, stress resistance had to take place (e.g., 8,21). In many of these early studies, researchers had discovered evidence of adaptive behavior; however, the nomenclature for labeling these results as indicative of resilience had not yet emerged.
The historical roots of resilience can be traced to early programs of research on individuals with schizophrenia and on persons exposed to parental mental illness, extreme stress and poverty, as well as on the functioning of individuals who experienced traumatic occurrences earlier in their lives 7,15,22,23. Early investigations of severely disordered schizophrenic patients were focused primarily on understanding maladaptive behavior, and the subset of patients who showed relatively adaptive patterns were considered atypical and afforded little attention. By the middle of the 20th century, researchers had discovered that people with schizophrenia with the least severe courses of illness were characterized by a premorbid history of a relative competence at work, good social relations, marriage and the capacity to fulfill responsibility (see 23). In a parallel fashion, studies of children of mothers with schizophrenia played a crucial role in the emergence of childhood resilience as a major theoretical and empirical topic 16,19,24.Additionally, Werner’s longitudinal study 17,18, that systematically searched for protective forces that differentiated children with healthy adaptation profiles from those who were comparatively less well adjusted, was a groundbreaking investigation. Evidence that many of these children experiencing great adversity thrived despite their high-risk status led to increasing empirical efforts to understand individual variations in response to adversity. Early empirical efforts were primarily focused on the personal qualities of “resilient children”, such as autonomy or high self-esteem 25. As work in the area evolved, however, researchers increasingly acknowledged that resilience may often derive from factors external to the child 8. Subsequent research led to the delineation of these sets of factors implicated in the development of resilience: (a) attributes of the children themselves; (b) aspects of their families; and (c) characteristics of their wider social environments 8,25.In recent decades, there has been a shift in the focus of empirical investigations; rather than searching for protective factors, researchers are increasingly striving to discover the mechanisms underlying resilient functioning 8. This focus on processes as opposed to identifying factors has enabled scientists to design prevention and intervention strategies that are developmentally sensitive for promoting resilience in persons experiencing significant adversity or trauma 26,27,28. Knowledge of the processes contributing to resilient functioning can enable prevention and intervention scientists to capitalize on periods of developmental change and transitions as unique opportunities for promoting positive adaptation during significant adversity or trauma 27,29. As S. Luthar asserted, “it is far more prudent to promote the development of resilient functioning early in the course of development rather than to implement treatments to repair disorders once they are already crystallized” 7. Randomized control trial (RCT) preventive interventions may be conceptualized as true experiments in altering the course of development 30, thereby presenting opportunities to test existing developmental theories as well as to provide insights into the etiology and course of positive adaptational outcomes in individuals experiencing significant adversity 8,31.As research on resilience has evolved and transformed over the years, it has become clear that the attainment of positive adaptation in the face of significant adversity involves a developmental progression; new vulnerabilities and challenges and/or strengths and opportunities often emerge with changing circumstances over the life course 8. Resilience is not something an individual “has” – it is a multiply determined developmental process that is not fixed or immutable. Hence, it is important to conduct longitudinal studies of the determinants of resilient functioning. In this regard, longitudinal studies on resilience should focus not only on assessing the stability of the construct over developmental time, but also on the ability of formerly resilient individuals to “bounce back” or to recover positive functioning after experiencing difficult periods and achieve their prior resilient adaptation 32. Moreover, since resilient adaptation may be achieved at any point in the life cycle, there is a need for research on the achievement of positive outcomes at different points in development, including in adulthood and in later life 8.A MULTILEVEL PERSPECTIVE ON RESILIENCEUntil the past decade, the empirical study of resilience predominantly focused on behavioral and psychosocial correlates of, and contributors to, the phenomenon and did not examine biological correlates or contributors 8,10,11. These studies were undertaken prior to the inception of modern techniques for examining the molecular genetic, neural, and biological correlates of human behavior and development.Evidence from earlier variable-oriented and person-oriented investigations of resilience converge on a short list of attributes of child and environment that turn out to be well-established general correlates of competent adaptation and psychopathology. Although there were methodological flaws and limitations in the early studies 14, more contemporary investigations nonetheless continue to corroborate the factors associated with resilient functioning: (a) close relationships with competent and caring adults in the family and community; (b) self-regulation abilities; (c) positive views of self; (d) motivation to be effective in the environment (i.e., self-efficacy and self-determination); and e) friendships and romantic attachments with prosocial and well-regulated peers 12. Problem-solving skills, foresight in planning, and a future orientation (all linked to executive functions), active coping strategies, and the capacity to confront fears directly, minimizing denial, disengagement, and avoidant coping have all been associated with resilient functioning 7,12,14. Moreover, optimism, positive emotionality, perceiving stressful occurrences in less threatening ways and the ability to reframe adverse experiences in a positive vein, spirituality, and being able to find meaning amidst trauma have each been linked to resilience 33.Undoubtedly, the relative neglect of biology as relevant to developmental theorizing on the unfolding of adaptive behavioral outcomes in the face of adversity was primarily due to the paucity of information that existed about the structural and functional organization of the brain 34,35,36. There simply was not enough knowledge about brain development and function to articulate their role in the genesis and epigenesis of normal and deviant mental processes, let alone in their contribution to the development of resilient adaptation 33.Most of what is known about the causes, correlates, course, and consequences of resilient functioning in the face of adversity have been gleaned from investigations that focused on relatively narrow domains of variables 7,8. Yet it is apparent from the questions addressed by developmental psychopathologists that progress toward a process-level understanding of resilient adaptation will require the implementation of research designs and strategies that call for the simultaneous assessment of multiple domains of variables both within and outside of the developing person 11.
In the past decade, a number of scientists have urged researchers to incorporate neurobiological and molecular genetic assessments into their investigations of the developmental pathways to resilient functioning 10,11,37. Technological advances in molecular genetics, neuroimaging, magnetoencephalography, electroencephalographic (EEG) recording, and hormonal assay techniques have made it more feasible to conduct research on the development of resilience from a multilevel perspective 11,12.In addition, the advent of modern neuroscience, along with its many associated subdisciplines, represents an unprecedented opportunity to augment current conceptual and methodological approaches to the study of resilience. Regardless, it is critically important to keep in mind that biological domains do not function independently; rather, more commonly the functioning of one system influences the functional properties of one or more other systems, through a developmental cascade of bidirectionally influenced processes 38. Given this increasing recognition of the importance of considering many levels of interdependent processes simultaneously, in order to advance the understanding of a multifaceted phenomenon such as resilience, it is incumbent upon resilience researchers to meet the challenge of simultaneously incorporating multiple levels of analysis both across and within systems 39. Biological and psychological domains are both essential to include in basic research on resilience and in resilience-promoting interventions. Each level both informs and constrains all other levels of analysis. Moreover, the influence of levels on one another is almost always bidirectional.Because different levels of analysis constrain other levels, as scientists learn more about multiple levels of analysis, resilience researchers conducting their work at each level will need to develop theories that are consistent across all levels. When disciplines function in isolation, they run the risk of creating theories that ultimately will be incorrect, because vital information from other disciplines has either been ignored or is unknown. Just as is the case in systems neuroscience 40, it is critical that there be an integrative framework that incorporates all levels of analysis about complex systems in the development of resilience 11,36.Resilience in maltreated children: from single-level to multilevel investigation
Growing up under conditions of child maltreatment constitutes a profound immersion in severe stress that challenges and frequently impairs development across diverse domains of biological and psychological functioning 41. The ecological conditions associated with maltreatment represent a severe deviation from the average expectable environment. Maltreated children are likely to manifest atypicalities in neurobiological processes, physiological responsiveness, emotion recognition and emotion regulation, attachment relationships, self-system development, representational processes, social information processing, peer relationships, school functioning, and romantic relationships 41. Accordingly, maltreated children are likely to develop a profile of relatively enduring vulnerability factors, placing them at great risk for future maladaptation and psychopathology.Nonetheless, not all individuals who have been abused and neglected succumb to the extreme adversity in their lives. Investigation of how some maltreated individuals cope adaptively despite experiencing significant stress and trauma offers an opportunity to discover processes at multiple levels of analysis that are likely to be germane to effective coping in the face of adversity, yet less readily detectable under more normative stress exposure 42. Discovering how maltreated children develop and function resiliently despite experiencing a multitude of stressors offers considerable promise for elucidating developmental theories of coping and for prevention and intervention.In a longitudinal investigation of the pathways to resilience in maltreated children, we sought to ascertain if there were different pathways to resilient functioning in maltreated and non-maltreated children (both from comparable low socioeconomic backgrounds) and to explore whether there were differences between these groups in resilience, recovery of function, or decline in functioning over the 3-year period of the study 32. Maltreated children demonstrated greater dysfunction than non-maltreated children on several indicators of resilient functioning (e.g., competence with peers, behavior problems, school functioning, relationships with adult caregivers). Moreover, many of these deficits persisted across 2 or 3 consecutive years of assessment. Furthermore, across each of the 3 years, maltreated children exhibited a lower level of resilient functioning than did the non-maltreated children. Additionally, the continuity of maladaptive functioning displayed by maltreated children across the course of this longitudinal study was substantial. Taken together, these findings underscore the deleterious impact that maltreatment experiences exert on competent functioning and attest to the non-transient nature of their influence.In this study, we also constructed pattern groups based on the three consecutive yearly assessments of resilient functioning in maltreated and non-maltreated children. Inspection of these pattern groups revealed that there was a significantly greater percentage of maltreated children than non-maltreated children in the low resilient functioning pattern group (40.6% vs. 20%). Furthermore, a greater percentage of maltreated (9.8%) than non-maltreated children (1.3%) displayed zero competence indicators, thereby reflecting an absence of resilient strivings across the 3 year study period. Garmezy 16,24 consistently emphasized that most children maintain the ability to display some resilience strivings in the presence of chronic and serious adversity. The complete absence of resilient strivings in nearly 10% of the maltreated children is cause for great concern, as self-righting tendencies are vital characteristics of all living organisms. The consistent absence of such strivings throughout the duration of the investigation is quite aberrant and alarming.We also examined factors that contributed to the development of resilient functioning in the groups of disadvantaged maltreated and non-maltreated children. For the maltreated children, the major predictors of resilient functioning were the personality characteristics of ego overcontrol (i.e., the ability to monitor and control impulses and regulate affect) and ego resiliency (i.e., the degree of relative flexibility in regulating affect and behavior to meet situational demands), and positive self-esteem. In contrast, for the non-maltreated children, positive relationships with their mother and other adult caregivers and ego resiliency played prominent roles in the prediction of adaptive functioning. Given the high percentage of insecure and disorganized attachments in maltreated youngsters 43, it makes sense that relationship factors would be more vital to the attainment of resilience in the disadvantaged non-maltreated children.Personality characteristics and self-system processes were more important in achieving resilient adaptation in maltreated children. Specifically, the self-system variables of self-reliance and self-confidence, in concert with interpersonal reserve (i.e., ego overcontrol), appear to bode well for the development of resilient adaptation in maltreated children. Through adopting a more reserved, controlled, and rational way of interacting and relating (i.e., resilient overcontrol), maltreated children who function in a resilient fashion may be more attuned to what is necessary for successful adaptation in their adverse home environments. It is conceivable that their more overcontrolled style may protect them from being targets of continued maltreatment incidents. In contrast, the more affectively expressive style of resilient undercontrollers may not be well suited for successful adaptation in maltreating environments, because such styles may provoke attention and reaction from others that could result in greater risk for maltreatment 44.Following the completion of this longitudinal investigation of the psychosocial processes underlying resilience in maltreated children, we initiated two multilevel studies. The ecological-transactional perspective that undergirds this research inherently takes into account multiple levels of analysis, and allows for combining biological and psychological mechanisms within the same framework 3,4. This perspective does not ascribe ascendancy to any level of analysis over another, and it encourages loosening of conceptual boundaries between nature and nurture and biology and psychology 45,46,47. This theoretical perspective thus provides a ready-made structure for the integration of a multilevel perspective into resilience.In the first multilevel investigation of resilience, emotion regulation, and hemispheric EEG asymmetry in maltreated and nonmaltreated children from high-stress low socioeconomic backgrounds, we hypothesized that the positive emotionality and increased emotion regulatory ability associated with resilient functioning would be associated with relatively greater left frontal EEG activity 48. A large body of literature concerning the meaning and correlates of hemispheric asymmetries in EEG activity has suggested that this ubiquitous phenomenon indexes a neural system that has emotion-specific influences whereby the two hemispheres of the cerebral cortex have been found to be differentially involved in emotion 48. Specifically, the left hemisphere is associated with positive emotions/approach behavior and the right hemisphere is linked with negative emotions/withdrawal behavior. Emotions, and in particular positive emotion and good emotion regulatory abilities, have consistently been associated with resilient adaptation 18,49,50. Thus, the potential connection of hemispheric EEG asymmetry with resilience lies in their common linkages with emotion and emotion regulation.EEG asymmetry across central cortical regions distinguished between children with high and low resilient functioning, such that left hemisphere activity characterized those maltreated children who were adapting resiliently based on our competence composite index (e.g., good peer relations, adapting successfully to school, low levels of depressive symptomatology, low externalizing and internalizing psychopathology) 51. Moreover, a behavioral measure of emotion regulation, based on 35 hours of observation of the children, significantly contributed to the prediction of resilience in maltreated and non-maltreated children.The investigation of a neural-level phenomenon such as hemispheric EEG asymmetry in the context of resilient adaptation reminds us that there is certainly no one single characteristic that will be ascendant in the process of resilience over the course of development. Resilience is a dynamic, interactive process between multiple levels across time, none of which holds primary importance at any given moment. However, viewed across development, the relative importance of various biological and psychological processes, although inevitably interrelated, may also vary across development.In another multilevel investigation conducted in our laboratory, resilient functioning in maltreated and non-maltreated low-income children in relation to the regulation of two stress-responsive adrenal steroid hormones, cortisol and dehydroepiandrosterone (DHEA), as well as the personality constructs of ego resiliency and ego control, was examined 52. The steroid hormones we chose to investigate as potential predictors of resilience are the two primary adrenocortical products of secretory activity of the hypothalamic-pituitary-adrenal (HPA) axis. The capacity of individuals to elevate cortisol levels in response to exposure to acute trauma is important for survival 2. DHEA exerts an impact upon a diverse array of biological actions, including effects on the immune, cardiovascular, endocrine, metabolic, and central nervous systems 53.As in the previous single- and multilevel research on the pathways to resilient adaptation described above, we utilized a composite measure of resilience that included multi-method, multi-informant assessments of competent peer relations, school success, and low levels of internalizing and externalizing symptomatology. We found that ego resiliency and ego overcontrol and the adrenal steroid hormones associated with stress (i.e., cortisol and DHEA) made independent and non-interactive contributions to resilience. Although operating at different levels of analysis, behavioral/psychological and biological factors each made unique contributions to resilience.Prolonged stress, as is often the case in child maltreatment, can lead to allostatic load, characterized by cumulative physiological dysregulation across multiple biological systems, through a cascade of causes and sequelae that can change the brain, organ systems, and the neurochemical balance that undergirds cognition, emotion, mood, personality, and behavior 54,55. Allostatic load is thought to occur when the adaptation to stress necessitates that the responses must be maintained over sustained time periods. Allostasis and allostatic load can be conceived as embodying a general biological principle – namely that the systems that help the body adapt to stress, and serve a protective function in the short term, also may take part in the development of pathophysiological processes when overused or managed ineffectively.We found that higher morning levels of cortisol were related to lower levels of resilient strivings for the non-maltreated children. High basal cortisol may indicate that non-maltreated children are experiencing greater stress exposure and, consequently, are constrained in their ability to adapt competently. Within the group of maltreated children, differences in cortisol regulation were found as a function of the subtype(s) of maltreatment experienced. Physically abused children with high morning cortisol had higher resilient functioning than physically abused children with lower levels of morning cortisol. The positive role of increased cortisol for physically abused children is divergent from the more general pattern of higher cortisol being related to lower resilient functioning as we discovered in the non-maltreated and sexually abused children in this study.Prior research on neuroendocrine regulation has indicated that physically abused children generally exhibit lower levels of morning cortisol secretion 56. It may be that the subgroup of physically abused children who were able to elevate cortisol to cope with the life stressors was demonstrating a greater striving for resilient adaptation. In contrast, the larger subgroup of physically abused children with lower levels of morning cortisol may have developed hypocortisolism over time in response to chronic stress exposure (i.e., allostatic load) 57. As a result, for these children there may be a diminished capacity to mobilize the HPA axis to promote positive adaptation under conditions of ongoing stress. Additionally, we found that the very low level of resilience among sexually abused children with high basal cortisol may be a product of their different traumatic experiences and consequences of chronic excessive vigilance and preoccupation, with commensurate HPA axis hyperarousal 52.Finally, we also discovered that maltreated children with high resilient functioning exhibited a unique atypical pattern of a relative DHEA diurnal increase. Maltreated children who have the capacity to elevate DHEA over the course of the day may be better equipped to cope with the demands of high chronic exposure to stress and to adapt competently. In contrast, the non-maltreated children who functioned resiliently did not exhibit the pattern of diurnal DHEA increase; instead they displayed the lowest levels of DHEA across the day.Gene-environment interaction and the molecular mechanisms that promote resilient functioning in maltreated children
Recent years have witnessed a renascence of interest in investigating the interaction between genes and environmental pathogens in the development of psychopathology and resilience 58,59,60. From a genetic perspective, resilience can be conceptualized as the extent to which persons at genetic risk for maladaptation and mental disorder are not affected 61. Additionally, there may be genetic contributors to resilient adaptation that protect some individuals in families where there is a high genetic loading for developing maladaptation and mental disorder from succumbing to these deleterious outcomes 58. Moreover, genes are likely to serve a protective function against environmental insults for some individuals. Thus, it is apparent that genetic influences on maladaptation and psychopathology operate in a probabilistic and not in a deterministic manner.In gene-environment interaction (GxE), environmental experiences moderate genetic effects (or vice versa) on normal, psychopathological, and resilient developmental outcomes. For example, genetic effects on functioning outcomes may be observed only under certain environmental contexts or in conjunction with particular histories of experience; conversely, experience may only relate to outcomes among persons with specific genetic characteristics 62.The majority of GxE studies have investigated polymorphisms in monoamine oxidase A (MAOA) and serotonin transporter (5-HTT), two of the primary genes implicated in the maturation of the early developing brain and in mood, behavior, and responsiveness to stress 58. The variability exhibited in children’s responses to the environmental hazard of child maltreatment suggests that this heterogeneity may be within the hemisphere of genetic influence 59. The experience of child maltreatment has proven to be a strong environmental pathogen that has generated a number of provocative findings which have contributed to engendering interest in research on GxE (59,60; for meta-analyses, see 65,66).Caspi and colleagues 62,63 demonstrated GxE effects in a large sample of adults who had experienced severe early child maltreatment. Specifically, Caspi et al 58 found that adult males who were maltreated early in development and who possessed the low activity allelic variant of the MAOA gene evidenced higher levels of antisocial and aggressive symptomatology than did those individuals who were maltreated early and who had the high activity variant of MAOA. The latter group demonstrated lower levels of antisocial and aggressive symptoms 62 than did maltreated adults with the low activity variant of MAOA. In a subsequent investigation, Caspi et al 63 discovered that adults who experienced severe maltreatment in childhood and who possessed the short (s/s) variant of the 5-HTT gene exhibited higher levels of depressive symptoms than did adults who had the long variant (l/l) of the 5-HTT gene and had been maltreated as children. In contrast, adults in the latter group had significantly fewer depressive symptoms than did maltreated adults with the short allele variants 63. Thus, it is conceivable that the high activity MAOA gene polymorphism and the long variants of the 5-HTT gene may confer protection against antisocial disorder and depression to adults who have been severely maltreated in their childhood.In our laboratory, we conducted a multigenic study examining the interaction between polymorphisms of 5-HTT and MAOA genes in a large sample of maltreated children in relation to depressive symptomatology 67. Adolescents from low socioeconomic backgrounds with a history of child maltreatment or no such history were administered a semi-structured diagnostic interview for mental disorders; moreover, these adolescents provided buccal cells for genetic analysis. Heightened depressive symptoms were found among extensively maltreated youth with low MAOA activity. Among comparably maltreated youths with high MAOA activity, self-coping strategies related to lower depressive symptoms. The finding that self-coping strategies and high MAOA activity were related to lower depressive symptoms calls to mind results from a number of our studies on resilience in maltreated children. Specifically, self-reliance and self-determination were found to be predictors of resilient functioning in maltreated children 32. It is conceivable that the maltreated children with positive self-system characteristics who functioned resiliently also may have possessed polymorphic variants of genes (such as high MAOA activity) that served a protective function against maladaptation.Sexual abuse and the 5-HTT short/short genotype predicted higher depression, anxiety, and somatic symptoms. This GxE interaction was further moderated by MAOA activity level. Specifically, we found that sexually abused adolescents with one or two copies of the 5-HTT short allele had significantly reduced levels of internalizing symptoms if they also had the high activity version of the MAOA gene 67.We also have begun to decipher co-actions across multiple levels of analysis through incorporating genetic and multiple physiological measures in our multilevel research on pathways to resilience in abused and neglected children. For example, in a longitudinal investigation that is currently underway in our laboratory, we are employing a multiple-levels-of-analysis approach to examining the course of trauma-related psychopathology in maltreated children, as well as the multilevel processes that contribute to resilient outcomes. In addition to genotyping relevant candidate genes, we have incorporated multiple measures of neurophysiological responses to classes of emotion stimuli, and hormonal, neurocognitive and behavioral functioning. The field can no longer afford to continue the artificial distinction among genetics, neurobiology, and behavior in research on the determinants of resilience.Neural plasticity and resilience: some potential linkages
Experience-expectant and experience-dependent mechanisms of neural plasticity are integral to the very anatomical structure of cortical tissue and cause the formation of the brain to be an extended malleable process 65,66,67. Developmental psychopathologists and neuroscientists can utilize this knowledge as an avenue for understanding the vulnerability and protective processes of brain development as contributors to the genesis and epigenesis of psychopathology and resilience. Moreover, because the mechanisms of plasticity cause the brain’s anatomical differentiation to be dependent on stimulation from the environment, it is clear that the cytoarchitecture of the cerebral cortex is shaped by input from the social environment. Because the human cortex is only diffusely structured by the genetic plan, and because its eventual differentiation is highly reactive to the active coping strategies of the individual in a particular environment, it is highly likely that both normal, abnormal, and resilient outcomes of this process would encompass a diverse range of cortical network anatomies and individual personalities.Analogous to neural plasticity that takes place in response to brain injury 68,69,70,71, resilience can be viewed as the ability of an individual to recover after exposure to adversity or trauma 9,32. According to this view, adversity is thought to exert a damaging effect on one or more neural substrates, and mechanisms of neural plasticity bring about recovery in an individual. This might lead to the conclusion that certain individuals, classified as resilient, may have some increased innate capacity (i.e., plasticity), above and beyond normative levels, to recover from environmental insults that impact the brain. This view of resilience conceives of adversity in the environment as “bad” for the brain, with recovery as an innate property of the brain itself. This perspective, however, does not consider the impact of a positive environment (e.g., presence of social supports), or of the individual’s active attempts at coping, or of protective/plasticity genes, on such recovery.Another conceptualization of resilience would be one of greater than normative resistance to the impact of environmental adversity on the brain, such that resilient individuals may not succumb to the potentially damaging effects that adversity may have on the brain and other biological systems. This view of brain-adversity interaction would not strictly be classified as involving neural plasticity. Thus, for these individuals, the term recovery of function may not apply, in that they did not “lose” function at all.The rapid growth in sophisticated techniques that permit imaging of the brain directly has resulted in the availability of a variety of methodologies to developmental psychopathology researchers; many of these methods could be utilized to examine neural plasticity, as well as brain structure and function, in detail. These new tools make it possible to now undertake empirical investigations of the relation between neural plasticity and resilience, perhaps enabling an examination of the direct linkage of these two processes. Questions about how neural plasticity may play a role in the development and maintenance of resilient functioning could be addressed, as well as whether the mechanisms of neural plasticity may operate differently in individuals classified as resilient.Among the compelling questions about resilient adaptation that could potentially be addressed utilizing brain imaging methodologies are: (a) Is brain structure and function different in maltreated and non-maltreated children functioning resiliently, matched on experiences of adversity? (b) Is the brain structure and function of resilient individuals who have experienced adversity different from normal children reared in non-adverse environments? (c) Are particular areas of the brain more likely to be activated in resilient than in non-resilient functioning during challenging or stressful tasks? (d) What aspects of brain structure and function differentiate individuals who function resiliently, despite experiencing early adversity, from those who function in a non-resilient fashion and who encounter adversity early in life (i.e., what is the role of early experience?) e) Are there sensitive periods beyond which the achievement of resilience is improbable or is resilience possible to achieve across the life span? and f) Are there changes over time in brain structure and/or functioning in individuals classified as resilient that may reflect processes of neural plasticity? The inclusion of neuroimaging techniques to the existing predominantly psychological approaches to charting the pathways to resilience, along with the additional biological and molecular genetic methodologies discussed earlier in this paper, could result in many exciting discoveries about the complex processes that eventuate in competent outcomes despite the experience of significant adversity.Aside from investigating the proximal relation between resilience and neural plasticity, there are several neurobiologically mediated processes (e.g., cognition, neuroendocrine functioning) that have a direct relation to resilient outcome 14,51. Although such processes exert an impact on resilient functioning, neural plasticity may, to some degree, be the common, underlying mechanism that mediates the relation between such processes and resilience.Resilience-promoting interventions: a multilevel perspective
Research on resilience has substantial potential to guide the development and implementation of interventions for facilitating the promotion of resilient functioning in diverse high-risk populations that have experienced significant adversity 27,72. Such interventions should target protective and vulnerability forces at multiple levels of influence – culture, community, family, and the individual.
Although several of the interventions that have been implemented have employed a multifaceted approach in order to ensure sensitivity to the diverse transactions between children and their environmental contexts, to our knowledge there have been very few interventions that have included biological assessments as part of the pre-post evaluation battery. Because one of the primary objectives of the field of prevention science is to intervene in the course of development to foster the recovery of function and to promote resilient adaptation in individuals at high risk for psychopathology 6, it is now essential to utilize a multiple-levels-of-analysis perspective ranging from DNA sequences to culture in research evaluations aimed at assessing the efficacy of RCT interventions whose goal is to foster the development of resilient adaptation.There are at least two reasons for the dearth of attention to biological processes in the evaluation of preventive interventions with children and adolescents. This lack of attention may partly originate from a tradition in developmental psychology of measuring biological processes as indices of heritable, constitutional individual differences reflecting the neurobiological bases of temperament 73. This tradition encourages beliefs that biological processes are either not malleable or are more refractory to positive change as a result of experience. Because there are bidirectional relations between different levels of biological and psychological organization, it is essential to recognize that experience also influences biology 68,74. Evidence for neurobiological reorganization in response to alterations in the environment may be less apparent in normative populations where there likely is greater stability in supportive milieus; however, investigations of individuals reared in extreme environmental conditions should enable us to more clearly isolate the components of these diverse systems, thereby shedding light on the bidirectional effects of experience and neurobiology.Random assignment to adversity or trauma is not possible, but random assignment to intervention is. If biological systems recover in response to the intervention, then this provides support for arguments that the systems under study are sensitive to environmental input during development. Furthermore, if randomized interventions alter neurobiological systems associated with disorders, and it can be shown that they mediate changes in psychosocial and behavioral functioning, then this fosters a better understanding of the neurobiological bases of the disorder. Moreover, preventive interventions may contribute to recovery or repair of biological sequelae in ways that have only begun to be understood. Improved comprehension of the neurobiological processes that increase risk of maladaptive development may also suggest novel targets for preventive intervention. Thus, it is important for prevention scientists to investigate the means by which changes in experience and psychological functioning resulting from preventive interventions may modify biological processes.Now that animal studies have demonstrated that experience can exert impacts on the microstructure and biochemistry of the brain 75, a vital role for continuing neural plasticity throughout epigenesis in contributing to the recovery from various forms of maladaptation and mental disorder may be suggested. There is growing evidence in the animal literature that efficacious interventions modify not only maladaptive behavior, but also the cellular and physiological correlates of behavior 76,77. Successful preventive interventions may alter behavior and physiology through producing alterations in gene expression that create a new structural reorganization in the brain 76. One important goal of preventive intervention research is to identify periods of development when a specific intervention may be more efficacious so that the intervention can be targeted to that period. A goal of preventive intervention work that includes measures of neurobiological processes is to better identify sensitive periods for intervention 78.Determining the multiple levels at which change is engendered through RCT prevention trials will provide more insights into the mechanisms of change, the extent to which neural plasticity may be promoted, and the interrelations between biological and psychological processes in maladaptation, psychopathology, and resilience 79. Moreover, preventive interventions with the most in-depth empirical support, based on integrative multilevel theories of normality, psychopathology, and resilience, can be implemented in effectiveness trials in community or real-world settings to reach the broadest number of people and prevent, alleviate, and ultimately cure, suffering from mental disorders 80. Furthermore, the inclusion of biological assessments in evaluations of interventions designed to foster resilience will enable scientists to discover whether the various components of multifaceted interventions each exert a differential impact on separate brain systems. It is thus possible to conceptualize successful resilience-promoting interventions as examples of experience-dependent neural plasticity.Finally, although the consensus is that resilience is a dynamic developmental construct that, theoretically, is possible throughout the life course, it nonetheless is important to ascertain whether the timing of resilience-promoting interventions is a crucial variable that merits consideration. Specifically, it will be extremely important to know whether resilience-promoting interventions are more effective when implemented in the early years of life. Likewise, are such interventions more likely to achieve their goal of promoting resilience if they are instituted as closely as possible to the identification of the adverse event(s) or experience? The incorporation of a multiple-levels-of-analysis perspective will enable scientists to learn whether, for example, resilience-promoting interventions implemented in the early years of life are better for brain development and functioning, even if improvement occurs in individuals who receive resilience-facilitating interventions later in life or receive their interventions further removed in time from their adverse event(s) or traumatic experiences.CONCLUSIONSIt is important to note that the call for a multilevel perspective in resilience research and resilience-promoting interventions − that includes the criticality of conducting genetic and neurobiological, as well as behavioral, assessments − does not reduce resilience to biology, let alone to a single biological variable. The inclusion of a multilevel perspective on resilience should not hearken scientists and clinicians back to the time when some espoused the view that they were “invulnerable” children. The incorporation of a multilevel perspective into research on resilience still requires adherence to a dynamic, transactional view that respects the importance of context.We are in the midst of a truly exciting period for research on the pathways to resilient functioning in individuals who have experienced great adversity and trauma. The advances in genomics, epigenetics, brain imaging, and hormonal and immunological assay techniques will make important contributions to propelling increased knowledge about the developmental processes leading to resilience 11,12. Such enhanced understanding has great potential for the development and implementation of novel, perhaps even individualized, resilience-promoting interventions for high-risk children and adults who are not functioning well due to experiences of adversity and trauma. In order to comprehend fully how individuals achieve resilient functioning in the face of adversity, it is incumbent upon us to investigate it with a commensurate level of complexity.AcknowledgementsWork on this article was supported by grants from the National Institute of Mental Health (MH083979) and the Spunk Fund, Inc.
No comments:
Post a Comment