Wow. This paper has, perhaps, the most convoluted and self-reflexive abstract I think I have ever seen. And yet I suspect that is the point - the author is using her own brain function as the research design for a qualitative study of the subject ("recursive, intrinsic, self-reflexive as de-and/or resubjective always evolving living research designs").
The author employs the Möbius Strip as an image for her ideas.
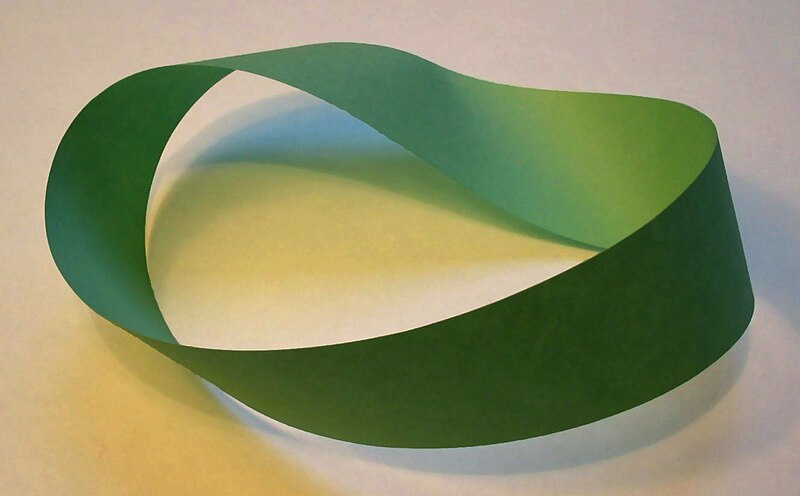
A Möbius strip made with a piece of paper and tape. If an ant were to crawl along the length of this strip, it would return to its starting point having traversed the entire length of the strip (on both sides of the original paper) without ever crossing an edge.
Full Citation:
Reinersten, AB. (2013, Jul 12). Welcome to My Brain. Qualitative Inquiry, XX(X); 1-12. doi: 10.1177/1077800413489534
Abstract
This is about developing recursive, intrinsic, self-reflexive as de-and/or resubjective always evolving living research designs. It is about learning and memory cognition and experiment poetic/creative pedagogical science establishing a view of students ultimately me as subjects of will (not) gaining from disorder and noise: Antifragile and antifragility and pedagogy as movements in/through place/space. Further, it is about postconceptual hyperbolic word creation thus a view of using language for thinking not primarily for communication. It is brain research with a twist and becoming, ultimately valuation of knowledges processes: Becoming with data again and again and self-writing theory. I use knitting the Möbius strip and other art/math hyperbolic knitted and crocheted objects to illustrate nonbinary . . . perhaps. Generally; this is about asking how-questions more than what-questions.
The article is available to read or download at Scribd, but here is a taste of the first couple of pages:
Introduction and the Möbius Strip
“So freedom of thought exists when I can have all possible thoughts; but the thoughts become property only by not being able to become masters. In the time of freedom of thought, thoughts (ideas) rule; but, if I attain to property in thought, they stand as my creatures.
If the hierarchy had not so penetrated men to the innermost as to take from them all courage to pursue free thoughts, that is, thoughts perhaps displeasing to God, one would have to consider freedom of thought just as empty a word as, say, a freedom of digestion.
According to the professionals’ opinion, the thought is given to me; according to the freethinkers’, I seek the thought. There the truth is already found and extant, only I must—receive it from its Giver by grace; here the truth is to be sought and is my goal, lying in the future, toward which I have to run.” (Stirner, 2012: Kindle locations 5514-5519).
Welcome to my brain. It is plastic, mentally creative, and physically adaptable just like yours if we want to. It is a chaotic noisy place wanting to produce results. I will not let one area dominate however. Also, there are places I do not want to go. Cortex- Hippocampus- learning and memory Cognition, emotional, sensory, bodily, social centers . . . —in the brain . . . So first; start with a long rectangle (ABCD) made of paper. Then give the rectangle a half twist. Third; join the ends so that A is matched with D and B is matched with C. Now you have created a continuous one-sided surface from this rectangular strip only by rotating one end 180° and attaching it to the other end. The brain is/has architecture (The Cortex) and neurons form networks forming larger networks processing information. Networks that for example allow us to recognize and code space, develop tools and navigate thus decide, make matter, and plan ahead. These are processes of orientation in/through space. Navigating and thinking about navigating simultaneously. Movements and moving and words as thinking tools: Complex processes of building complex representations of compass distances—learning and memory—measurements. And important: Thinking/planning also without direct sensory impulses: Thus having the ability to generate new ideas and ideas about the future too . . . in the brain. To live such complexity I turn to “knitting around” Möbius Band Scarves (Zimmerman, 1989) as you will see below. Very easy but not; I had to rehearse. Thus calming but not, product oriented nice and warm—comfortable—if I finish but also while doing.
As you now know, this nonorientable surface is called a Möbius Strip or Möbius Band, named after August F. Möbius, a 19th century German mathematician and astronomer, who was a pioneer in the field of topology. Möbius, along with his contemporaries, Riemann, Lobachevsky, and Bolyai, created a non-Euclidean revolution in geometry. Möbius strips have found a number of applications that exploit a remarkable property they possess: one-sidedness. Joining A to C and B to D (no half twist) would produce a simple belt-shaped loop with two sides and two edges—impossible to travel from one side to the other without crossing an edge. But, as a result of the half twist, the Möbius Strip has only one side and one edge, and I am the no-one-sided teacher/researcher/professor in education: a nonorientable surface with a boundary—architecture—Cortex—and you. Thus I/you/we must/can make choices and make knowledges matter. And sometimes I am forced or I force myself to go places. Qualia: the subjective experience of things, a property of something . . . its feel or appearance perhaps rather than the thing itself . . .: This is about finding the out there in the in here.
Here is what another teacher/researcher/professor, and this time in brain research at Center for Biology of Memory, Trondheim, Norway (CBM): www.ntnu.no/cbm, says about what he does, knows and thinks: “The Hippocampus is a part of the brain we know is relevant for learning and memory. There are brain structures there that are involved. The brain research area has exploded the recent years but still we are in the beginning of discovering general rules about how the brain processes information. Experimental evidence based science does not—must not/cannot—move too fast. We do not know that much and other so quickly. At least if we speak about evidence. Grounded scientific research is a privilege” (Interview, October 28th, 2011).
At CBM they started to study memory but ended up in studying sense of place/space: “Now we know that this sense is closely linked to memory. It is almost like a human GPS with grid cells in the part of the brain called the Entorhinal Cortex. Grid cells collaborate with other specialized nerve cells with complementary roles in the sense of place/space and direction. Together they build a map in the brain. And the brain uses this map to orient itself in both familiar and unfamiliar environments. Signals create a coordination system in which positions can be registered. They register our movements and are closely linked to our memory. The grid cells do not reflect signals that come in from the outside from any of our senses. The grid patterns are made by the brain itself. Therefore we can use the grid cells as a way of understanding how activity patterns emerge in the brain. The grid is opening up new possibilities to study how the brain stores information” (Moser & Moser, in Jacobsen, 2012).
“It is very difficult and risky to deduct anything directly between brain research and pedagogy, but one thing that we might say is that if you want to learn something different and other, it might be sensible to shift between places: Learning different things in different places that is” (Interview, October 28th, 2011).
Ethnomethodology is an approach to sociological inquiry as the study of the everyday methods that people use for the production of social order (Garfinkel, 1967). It is also called bottom-up microsociology and a member’s methods inquiring into common sense knowledge, self organizing systems, and situated natural language. The aim is to document methods and practices through which society’s members make sense of the world. It is in itself however not a method. It does not have a set of formal research methods or procedures.
Knitting is a repetitive visual spatial task. These tasks also include e.g. running and folding origami and can put our brain into the state of Theta (Retrieved Dec.7th. 2012). States of Theta can increase creativity, lower stress/anxiety and increase objectivity in difficult situations. Theta is also that state between falling asleep and waking up when we seem to have all of our best ideas. Because the brain is focusing on (literally) the task at hand, it isn’t as judgmental and has lower standards/barriers. Theta is nonjudgmental, more observant . . . objective? No but I try. And as you will see below, I try to hold my brain in my hands.
I and My Research . . . Brain . . . Questions
“Some things benefit from shocks; they thrive and grow when exposed to volatility, randomness, disorder, and stressors and love adventure, risk, and uncertainty. Yet in spite of the ubiquity of the phenomenon, there is no word for the exact opposite of fragile. Let us call it antifragile. Antifragility is beyond resilience or robustness. The resilient resist shocks and stays the same; the antifragile gets better” (Taleb, 2012, p. 3).
This article is therefore about developing recursive intrinsic self-reflexive as de- and/or resubjective always evolving living research designs. Inquiry perhaps full stop—me: An auto-brain—biography and/or a brain theorizing itself; me theorizing my brain. It is thus about theorizing bodily here brain and transcorporeal materialities, in ways that neither push us back into any traps of biological determinism or cultural essentialism, nor make us leave bodily matter and biologies behind. It is an attempt of seeing the real as/through/in its material-discursive coconstitutive complexity and produce research from within an ontology and epistemology where ‘matter and meaning are mutually articulated’ (Barad 2007, p. 152). It is about learning and memory cognition and experiment poetic and/or creative pedagogical science; learning ultimately pedagogy as movements in/through space.
It is brain research with a twist and becoming, ultimately valuation of knowledges process; a personal antifragile will born from knowledge. I use knitting and other, as you will see, to illustrate or rather live nonbinary. First, I will write more about research designing, second, about knitting Möbius bands. Third, I will philosophize a bit with Socrates, Meno and Plato: “Meno’s Paradox,” or “The Paradox of Inquiry” (Meno 80d-e) and Max Stirner (1806-1856) over learning and memory, one-sidedness, antifragility research, pedagogy, and will only to end in wonder. Eventually, this is a philosophical brain journey in which the question “how do you know” is more difficult but vital to ask than the “what do you know” question we traditionally have asked both ourselves and our students through years.
I treat theory, transcribed interview notes, pieces of art, creating knitting Möbius band scarves and myself as data (text). Data shapes and negotiate. Data are shaped and negotiated. There are data dilemmas—paradoxes. I am at hearing of the data; text and textuality. Thus I am (my own) data but as a “montage” in which “several different images are superimposed onto one another” (Denzin and Lincoln, 2003, p. 6). Several different texts: My brain. My knowledge of my ordinary affairs, of my own organized enterprises, as part of the same setting that makes it orderable.
It is broad and multifaceted and with open-ended references to any kind of sense-making procedure, a domain of uncharted dimensions my auto- brain- biography - ethnomethodology attempt.
I turn knitting, art into data and tool to see other and beget thinking; activate brain cells—circuits—inquiring minds; experiment—poetic—creative—pedagogical science—and language . . . making, de/re/constructing the world? I told you this was chaotic and noisy and my own moving sensations of sound touch taste and smell. And further, my amalgamations of images in order to make a very unique image of my own, and mine. Seeking to describe the common sense methods through which I produce myself as teacher/researcher. A member’s methods; my methods.